Phone: For support in Australia, call 1300 401 111 and select option 3 for Bp Allied. Next, select option 1 for Support or Option 3 for Training. For support in New Zealand call 0800 401 111 and select option 3 for Bp Allied. Next, select option 1 for Support or Option 3 for Training
MOC - Claimant Details
Any fields not required for the particular claim being lodged will be greyed out.
Claims for Children and Minors
Children and Minors who do not have their own Medicare card with the bank account registered against it MUST have the Claimant details filled in for the claim to be paid. The claimant must have their bank details registered with Medicare.
To help manage this process, the following prompts will appear.
If the Patient is under 15 years and Lodge Claim is clicked:
If the Patient is under 21 years:
Please refer to the Medicare rules to determine who qualifies as a Claimant and whether their registered bank account details can be used.
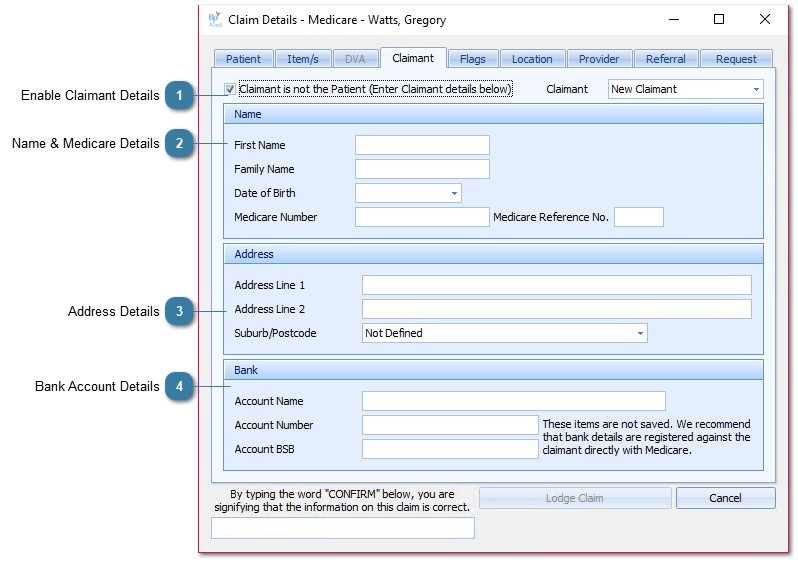
Enable Claimant Details
Tick to enable Claimant details to be entered. If there is no claimant saved against the client, Claimant will default to New Claimant with blank fields.
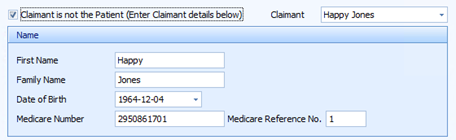
If there is a saved claimant, the first Claimant in the list will default into the fields.
Claimants can be added directly to and deleted from the client via the Client Details screen. Details on how are located here.
These five fields are Mandatory to be able to process a patient claim for a child or minor.
Claimant First Name The claimants first name when the patient and claimant are not one and the same. Required if claimant is not the patient 40 characters
Claimant Family Name The claimants family name when the patient and the claimant are not one and the same. Required if claimant is not the patient. 40 characters max.
Claimant Date of Birth The claimants Date of Birth, where a claimant is specified.
Claimant Medicare Number The claimants Medicare Card number when the patient and claimant are not one and the same.
Claimant Medicare Ref. The claimants individual Reference Number (found to the left of the claimants name on their Medicare card), when the patient and claimant are not one and the same. It is one (1) character and can not be a zero (0)
Claimant Address Line 1 First line of the temporary address to be used for the claim. Cannot be a PO Box Claimant address details must only be transmitted at the request of the claimant. These address details are temporary and must be used for that claim only. 40 characters max.
Claimant Address Line 2 Second line of the temporary address to be used for the claim. 40 characters max.
Claimant Address Locality The locality of the temporary address to be used for the claim.
Bank Account Name Used for EFT payments. The claimants bank or financial institution account name.
Bank Account Number Used for EFT payments. The claimants bank or financial institution account number.
Bank Account BSB Used for EFT Payments. The BSB code for the bank and branch where the account is held.
The Claimant's bank account details are not saved. It is our recommendation that the Claimant register their bank account details with Medicare rather than rely on payment to the account specified via this method.